
Your guide to understanding plantar fasciitis and how to treat it!
By Dr. Dina Elsalamony MD, MScPH
What is plantar fasciitis?
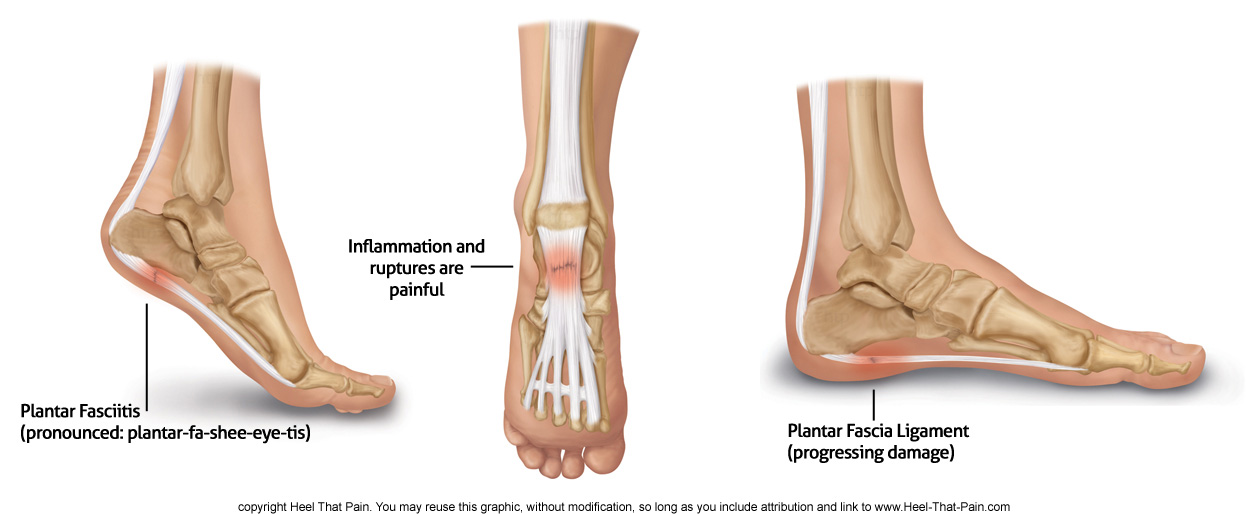
Plantar fasciitis is a common foot condition that involves pain, and occasionally, gait issues. The plantar fascia is a thick sheath of type 1 collagen that is located at the bottom of the foot, and its main responsibility is to act as a tension bridge, providing support for the arch of the foot, both while stationary or by absorbing the shock during movement.
Plantar fasciitis is characterized by stabbing, aching or burning pain that usually occurs during the first few steps in the morning or after long periods of rest, the pain tends to reduce after continuing to walk for more steps, however, it increases again when performing weight-bearing activities. In some cases, the pain could be substantial leading to changes in the person’s daily activities.
Plantar fasciitis is considered to be the most commonly reported cause of heel pain. In the case of runners, it is one of the most prevalent injuries, accounting for up to 8% of all running-related injuries. (1) While in the general population, the estimated prevalence ranges from 3.6% to 7%. (2,3) Women are affected by plantar fasciitis twice as often as men, with peak incidence occurring in women aged 40-60 years.
Various terms have been used to describe this condition such as tennis heel, jogger’s heel, and policeman’s heel. In some situations, it is mistakenly referred to by the general public as heel spurs, however this a misnomer since heel spurs is a different condition than plantar fasciitis, heel spur on its own usually is asymptomatic and doesn’t result in pain, on the other hand, many patients with plantar fasciitis do not have a spur.
Recommended for You:




Plantar fasciitis causes:
The exact cause of plantar fasciitis is unclear, and often a number of factors could contribute to the development of this condition. There is an established causation between some systemic issues and the development of plantar fasciitis, this could include traumatic, infectious, neurologic or arthritic conditions. However, biomechanical dysfunction of the foot is the most common explanation for plantar fasciitis as it is believed that repeated microtrauma (microtears) of the plantar fascia can result in chronic degeneration of its fibers, in addition to reduced nutritious blood flow to the impacted fascia, which makes it difficult for its cells to start repairing and healing.
Hence, plantar fasciitis is in fact a degenerative disorder and not an inflammatory one as the name suggests (fasci‘itis’ in Latin translates to inflammation), therefore this term is a misnomer as multiple studies have shown that this condition could happen with or without inflammation, and the more accurate term to use should be “fasciosis”, which means a pathology/abnormality in the fascia.
Plantar fasciitis risk factors:
The risk factors for plantar fasciitis could be categorized into factors related to your behavior, habits, environment, temporary changes in the body (extrinsic factors), and factors related to the inside of your body; how it is fundamentally built, and the core functions of your musculoskeletal system (intrinsic factors).
1. Extrinsic risk factors:
Active people, particularly runners, between the ages of 40 and 70 have the highest risk for developing plantar fasciitis. One of the main reasons for that is usually training errors; athletes tend to have recently abruptly increased the duration, intensity, or distance of their activity before developing plantar fasciitis pain.
Other risk factors include wearing the wrong footwear with poor arch support and soft soles, for example, athletes who train wearing minimally cushioned lightweight shoes (instead of heavier training flats) are at higher risk of developing plantar fasciitis. Additionally, indoor running on hard surfaces and hill workouts are also considered high-risk factors.
You are also at a greater risk of developing plantar fasciitis if you are pregnant, obese, have heel spurs, or in an occupation that requires prolonged standing and weight-bearing, this is due to the increased pressure on the plantar fascia which causes more micro-tearing.
2. Intrinsic risk factors:
Functional:
You could have a risk factor that is associated with your muscles, including weakness of the calf or foot muscles, and tightness of the hamstrings or the Achilles tendon which is the tendon that connect your heels to your calf muscles. Tightness of the Achilles tendon is found in almost 80% of cases. (4)
Structural:
In terms of your skeletal structure, low-arched or high-arched feet, leg-length discrepancy, and overpronation are all considered high risk factors for developing plantar fasciitis as they lead to increased tension on the plantar fascia.
Degenerative:
Aging can lead to loss of the fat padding of the foot, which could cause the plantar fascia to be more exposed and prone to repetitive trauma or injury.
Plantar fasciitis symptoms
People with plantar fasciitis usually complain of heel pain experienced mainly at the middle part of the bottom of the foot or at the heel or at both areas, the pain may also radiate from the heel upwards toward the leg in more severe cases.
This pain is primarily felt during the first few steps in the morning, usually, it is sharp in nature and is decreased when resting and lifting the leg up, or when slowly warming up by gently moving for more steps. Although, the pain usually comes back, in a duller aching form, after performing weight-bearing activity for an extended period, such as long walks, runs, or standing. In people suffering from a severe case of plantar fasciitis, pain may also be experienced after periods of prolonged sittings, it may cause the person to start limping or walk on their toes to avoid the pain.
The plantar fasciitis pain is often worsened by walking up the stairs, or by walking barefoot on hard surfaces. In occupations where the individuals are standing for long periods during the day, they experience much worse pain by the end of their working day, while in the case of runners, sprinting is typically what aggravates their pain.
The pain in most cases is felt in one foot, however, it is also possible to experience plantar fasciitis pain in both feet, studies have shown that up to 30% of cases could develop a similar or different level of plantar fasciitis bilaterally.(5)
Other symptoms than pain may also be experienced such as stiffness, redness, warmth or swelling of the inner side of the middle section of the bottom of the foot, or of the heel.
Plantar fasciitis diagnosis:
If you are experiencing this type of pain, it is vital to consult with your physician as soon as possible. The majority of plantar fasciitis cases resolves spontaneously or with conservative treatment within a year, however, early diagnosis and treatment are really important to enhance your recovery chances and prevent any further damage.
To accurately diagnose your condition and prescribe the appropriate treatment accordingly, your physician will carry out the following diagnostic measures:
- Condition history: your physician will enquire about the history of the pain; the period preceding the onset of the pain, and whether you had a sudden increase in a specific activity, started a new exercise, rapidly gained weight, had a recent change in your footwear or suffered any kind of trauma or accident.
- Physical examination: your physician will inspect your foot for any skin changes or structural deformities, they will perform a number of physical maneuvers to reproduce the pain and confirm its origin, in addition to checking your muscle tone, balance, coordination, and reflexes. Your physician may also conduct a full musculoskeletal examination and/or a vascular examination to eliminate any other potential causes for your heel pain.
- Laboratory tests: usually no blood tests are required to diagnose plantar fasciitis unless your physician suspects other causes for your pain or you are complaining of pain in both feet which might indicate other systemic issues that require blood tests to confirm.
- Radiography: plain x-ray may be needed to confirm the presence of a heel spur that over time could cause stress on the plantar fascia and eventually contribute to the development of plantar fasciitis. Other radiography tests such as MRI, CT scan, and ultrasound are rarely used and usually only requested if your physician suspects other conditions or serious complications of plantar fasciitis
Is there a cure for plantar fasciitis?
The condition of plantar fasciitis is usually self-limiting, if you were diagnosed with plantar fasciitis, case studies have shown that you probably have a 90% chance of recovery without any invasive or surgical measures. (6,7,8) However it is important to understand that the severity of the condition is different from one person to another, in addition to other factors, including the structure of your body, your lifestyle, and habits which all can affect how you would respond to various treatment, and how fast you would recover may vary from another person even if they have followed the same treatment as you.
In order to treat plantar fasciitis, It is very important to understand the possible causes and risk factors that could have played a role in the development of this condition, this will ensure addressing the root cause of the problem while treating the symptoms as well, which will result in a higher success rate and lower chances of recurrence. (9,10)
Plantar fasciitis treatments
The options for the treatment of this condition could be classified into the following:
1. Conservative treatment
These treatments could be done at home and are usually applied as the first line of treatment for the first six weeks, with the possibility of extending the regimen for another six weeks in some stubborn cases. For a greater chance of a speedy recovery, it is important to adhere to a combination of all the following conservative treatments simultaneously:
Orthotics
Shoe inserts or orthotics for plantar fasciitis can be used with existing shoes, the mechanism of pain reduction produced by the use of orthotics is accredited to the orthotics supporting function to the longitudinal arch of the foot. (11)
Orthotics for plantar fasciitis could either be bought over the counter without prescription or custom made to your specific foot. However, the disadvantage of custom-made orthotics is its high cost, usually ranging between 100-400 USD, while numerous studies have shown repeatedly that using prefabricated OTC orthotics is as effective in treating plantar fasciitis as custom-made ones. (12,13,14) In a systematic review study of 19 clinical trials that included 1660 participants, foot orthotics have been proven to reduce plantar heel pain in adults who have used them for a duration of (7-12) weeks. (15)
In another randomized treatment study, orthotics were found to be even significantly better than the use of heel cups, non-steroidal anti-inflammatory drugs, or cortisone injection. (16)
This does not mean to go out and buy any regular heel pad as they are useful only for mild shock absorption and do not provide support or structural control. Instead, it is strongly advised to buy orthotics that are specifically designed to treat plantar fasciitis by providing both shock absorption and strong support to your arch.
Try to find the densest material that is soft enough to be comfortable to walk on as highly supportive orthotics have been shown to greatly reduce pain in comparison to non-supportive soft orthotics.


Heel That Pain offers Heel Seats foot orthotics that utilized the revolutionary technology of fascia-bar, which is unique to Heel Seats and cannot be found in any other product on the market. During a double-blind clinical trial conducted by the University of Iowa on the fascia-bar technology, researchers concluded Fascia-Bar technology is two times as effective as the treatment method offered by a comparable leading brand orthotic. Those results were due to the remarkable ability of Heel Seats orthotics to absorb the impact during walking or standing, while also providing the ultimate support needed by lifting the affected plantar fascia to ensure its proper alignment.

The dense cushion used in the manufacturing of Heel Seats is made of soft Kraton, which provides the ultimate balance between being gentle on the foot and ensuring strong support for the plantar fascia. Heel Seats are very cost-effective as well, ranging from $24.95 – $34.95. This price range allows them to be affordable for most people providing a practical, accessible, and effective conservative treatment for anyone suffering from a non-severe case of plantar fasciitis, whether it is acute, chronic, or recurrent. Additionally, when it comes to adolescent athletes who may require a change of one or more arch support per season, due to their ongoing feet growth, Heel Seats provide an excellent alternative to overly-priced products on the market. Hence, 90% of customers have reported remarkable satisfaction with the result experienced after using Heel Seats.
Rest and activity alteration:
Resting is the first and most critical thing required for your plantar fascia to have time to heal. This means modifying your regular activity as much as possible to avoid any further tearing or damage. If you are an active person with a mild case, it is possible to continue doing other activities that don’t put stress on your feet, while trying to reduce the frequency or intensity of your usual exercise, it is advised to start by 50% of your usual time or distance, and increase 10% weekly. However, in the case of severe pain, complete immobilization may be necessary.
Icing:
Applying ice reduces the inflammation of the plantar fascia and the surrounding tissues. You should ice the bottom of your feet after completing any stretching or exercise. You can apply ice by using an ice bath for your feet, massaging, or ice packs. Heel That Pain offers a great choice of Ice Therapy Slippers that strap into your feet comfortably, providing a more convenient and practical method of icing, without having to worry about securing an icepack to your feet. The ice pack slippers will ice the entire surface of the bottom of your feet, reducing the swelling, pain, and inflammation caused by plantar fasciitis.
Medication:
Anti-inflammatory drugs play a critical role in treating plantar fasciitis, particularly OTC non-steroidal anti-inflammatory medications such as ibuprofen or diclofenac, as in addition to their analgesic effect, they also assist in the healing process of the plantar fascia. (17,18) However, it is critical to consult with your physician regarding taking these medications and to exercise caution in relation to the doses and duration of treatment due to their possible negative side effects on the kidney and the stomach.
Stretching exercises:
Numerous studies have suggested stretching as part of the conservative treatment of plantar fasciitis. This includes calf stretching exercises that could correct some of the functional risk factors such as tightness of the calf muscles and the Achilles tendon. Other stretches focused on strengthening the foot muscles are also strongly recommended. Stairs or curb stretches, wall stretches and towel stretches are some of the common stretching techniques used in the treatment of plantar fasciitis.
Night splints:
This treatment is usually suggested as a part of the conservative treatment regimen only for those with severe pain, otherwise, studies have suggested that it is specifically useful for those who had symptoms for more than a year. (19,20) The night splint is a type of brace that secures your foot in a neutral 90-degree angle position overnight since most people tend to sleep while in a plantar-flexed position which causes shortening of the plantar fascia. When wearing a night splint, your foot will be held in a position that allows constant stretching and lengthening to the Achilles tendon and plantar fascia, which in return will aid in the healing process. Additionally, the passive stretching provided by night splints prevents micro-tearing of the plantar fascia tissues during the first few steps taken in the morning.
Shoe change:
Most fashionable shoes do not provide enough support for the foot arch, also some people tend to wear shoes that are too small or do not fit properly to the length or width of their feet. All this could contribute to developing and aggravating the issue of plantar fasciitis. Generally, changing to lace-up shoes with well-cushioned thicker midsoles that are made of high-density materials, such as those found in a large number of high-quality running shoes, will aid in decreasing the pain experienced during standing or walking for an extended period of time. If you already own perfectly-fitting, high-quality running shoes that you have been using for a while, then maybe it is time to buy a new one, as studies have shown that running shoes lose a significant portion of their shock absorption with age. (21) If you have flat feet, then the best shoe type recommended in this case is motion control shoes, as they can provide longitudinal support to the arch and help with pain relief during activities. In one study (9)14% of patients cited that changing their footwear was the treatment that made the biggest difference for them.
2. Advanced treatment options
The following options may be suggested by your physician in the case of persistent symptoms that do not respond to conservative treatment:
Corticosteroid injection:
If you suffer from severe pain, or your symptoms did not improve after conservative treatment for 6 weeks, your physician would probably recommend continuing with the conservative regimen while also adding corticosteroid injections to the treatment. Your physician will administer the injections to your foot, under local anesthesia, and possibly guided by ultrasound to ensure the injection is in the most accurate spot and decrease the possibility of any complications. However, corticosteroid injections carry some undesirable side effects, such as the possibility of the rupture of the plantar fascia or fat pad atrophy.
Botulinum toxin injection:
Numerous studies have shown the promising results of ultrasound-guided injection of botulinum toxin type A, as it appears to significantly improve the pain and the overall foot function, (22,23) and in some trials even producing better results than corticosteroids injections without some of the possible side effects of steroid injections. (24)
Extracorporeal shock-wave therapy (ESWT):
This therapy uses high-pressure sound waves to send pulses to the affected nerves in the area to shut down their pain pathway which leads to pain reduction, additionally, the sound waves stimulate the blood flow to the tissues which helps with the natural immune response and the healing of the fascia. Several studies have concluded that ESWT is effective in fast pain relief and inflammation reduction, in addition to long-term tissue regeneration. (25,26,27)
Radiation therapy:
This non-invasive procedure is known as Topaz bipolar radiofrequency microdebridement, its mechanism relies on emitting bipolar radiofrequency pulses to the plantar fascia to help treat the damaged tissues and nerves. A number of studies (28,29) have shown this procedure yields successful results in significantly reducing pain for a duration of up to 6 months while having minimal side effects or complications when compared to the surgical option.
Cryosurgery:
This is a relatively new procedure, that is much less invasive than regular surgery, in which a small percutaneous incision is made to insert a cryoprobe (a prob that has a temperature of -70 C) to destroy the damaged tissues and encourage regeneration of healthy cells. A study of 137 feet has reported a success rate of 77% even after a duration of 2 years. (33)
Surgery:
This option is typically saved as a last resort for the treatment of plantar fasciitis in patients who don’t respond to conservative treatment for 6-12 months. The surgery is called fasciotomy and is performed by sectioning segments of the fascia using a regular surgical opening, or an endoscopic opening which usually leads to better results. Despite having a success rate of 70%-90%, (30,31) this surgery carries a number of possible short and long-term complications, particularly causing a strain on the longitudinal foot arch, which represents 50% of all the potential chronic complications associated with this surgery. (32)
Platelet-rich plasma injection:
It is believed that injecting the plantar fascia with plasma that has a high concentration of platelet may be beneficial in treating chronic plantar fasciitis, as it encouraging the natural healing process resulting in the resolution of the symptoms.
Iontophoresis:
This is a procedure where electric impulses are used at low voltage to push the corticosteroid applied topically into the soft tissues. Despite having been found to significantly improve the symptoms of plantar fasciitis in the short term, this procedure is not commonly used as it is neither time nor cost-effective, since it is required to be performed 2 to 3 times per week by a physical therapist, hence, it is usually reserved for the treatment of athletes who have the resources and the necessity to do so.
Plantar fasciitis prognosis and complications:
Although full recovery may take some time, this condition usually resolves spontaneously and with the use of the above-mentioned conservative treatment within a year for about 80% of the cases, and the cases that end up requiring surgery after failing to recover using the conservative treatment, are usually only around 5% of all plantar fasciitis cases. However, chronic plantar fasciitis can occur in some cases, particularly for those who ignored the condition for too long without seeking treatment or adopting any changes in their lifestyle. The long-term complications may include severe pain that leads to activity and movement restriction and a possible change in the way the individual bears their weight which could end up causing injury to the knee or hip joints.
On the other hand, surgery and some of the advanced treatment options for plantar fasciitis may cause a number of associated complications, such as reaction to anesthesia, infection, bleeding, nerve damage, and plantar fascia rapture. Hence, it is advised to exhaust all the conservative treatment options, before exploring any of the advanced options.
How to prevent plantar fasciitis
The best way to prevent plantar fasciitis from happening is by being educated on the condition and its risk factors. If you are an athlete or an active person, ensure sufficiently warming up and stretching before starting the activity, continue gentle stretching and ice down after finishing your exercise.
Be sure to always wear shoes that fit you perfectly, with dense cushions and support to the heel and foot arch, and if you are a runner, it is advised to change your running shoes every 250 to 500 miles, or you could alternate between two pairs of athletic footwear, to give the shoes cushiness a time to recover between exercises.
If you work in an occupation that requires standing on your feet or walking around for too long, try to invest in the appropriate footwear with the right sole and adequate padding that provides shock absorption and great support to your arch. Also, when possible, try to take sitting breaks and elevate your feet to decrease the time you are putting weight pressure on your plantar fascia and the surrounding structures. Icing after a long working day is another great way to relief any inflammation and allow any microtraumas to start healing naturally.
Final words of advice
Patience and discipline are critical when it comes to managing and treating plantar fasciitis. While having a high recovery rate, radical improvement can often take weeks or months to be felt, and requires understanding of what factors aggravate the condition in each specific case to be able to correct them.
Make sure to wear the right shoes with the adequate support needed, you could maybe use a quality-made orthotics that are convenient and provides dense cushion to the bottom of your feet.
If you are obese or have recently gained weight rapidly, it is really important to try to lose weight, since bearing large weight on your feet tend to cause a lot of stress and microtrauma to your plantar fascia.
Do not walk or exercise on hard surfaces, and do not start exercising without proper warm up and gentle stretching. Also, avoid any high impact exercises, particularly those that require jumping.
Make sure to give your body enough time to heal between activities, try to limit your activity to every other day, and in the case of your occupation requiring long periods of standing, your work place should accommodate your health needs and allow you time-off or change in work activity, since this condition could be considered as an occupation related injury in this case.
References:
1) Taunton, J. E. (2002). A retrospective case-control analysis of 2002 running injuries. British Journal of Sports Medicine, 36(2), 95–101. https://doi.org/10.1136/bjsm.36.2.95
2) 1. Dunn JE, Link CL, Felson DT, Crincoli MG, Keysor JJ, McKinlay JB. (2004). Prevalence of foot and ankle conditions in a multiethnic community sample of older adults. Am J Epidemiol, 159(5):491–8. [PubMed]
3) 2. Hill CL, Gill TK, Menz HB, Taylor AW. (2008). Prevalence and correlates of foot pain in a population-based study: the North West Adelaide health study. J Foot Ankle Res, 1(1):2. [PMC free article] [PubMed]
4) Singh D, Angel J, Bentley G, Trevino SG. (1997). Fortnightly review. Plantar fasciitis. BM, 315:172–5. [PMC free article] [PubMed]
5) Roxas M. (2005). Plantar fasciitis: Diagnosis and therapeutic considerations. Altern Med Rev, 10:83–93. [PubMed]
6) McPoil TG, Martin RL, Cornwall MW, Wukich DK, Irrgang JJ, Godges JJ. (2008). Heel pain–plantar fasciitis: clinical practice guildelines linked to the international classification of function, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther, 38(4):A1-A18. [Medline].
7) Davis PF, Severud E, Baxter DE. (1994). Painful heel syndrome: results of nonoperative treatment. Foot Ankle Int, 15(10):531-5. [Medline].
8) Gill LH, Kiebzak GM. (1996). Outcome of nonsurgical treatment for plantar fasciitis. Foot Ankle Int, 17(9):527-32. [Medline].
9) Wolgin M, Cook C, Graham C, Mauldin D. (1994). Conservative treatment of plantar heel pain: long-term follow-up. Foot Ankle Int, 15:97–102.
10) Martin RL, Irrgang JJ, Conti SF. (1998). Outcome study of subjects with insertional plantar fasciitis. Foot Ankle Int, 19:803–11.
11) Ribeiro AP, Trombini-Souza F, Tessutti VD, Lima FR, João S, Sacco IC. (2011). The effects of plantar fasciitis and pain on plantar pressure distribution of recreational runners. Clin Biomech (Bristol, Avon), 26:194–9. [PubMed]
12) Lee SY, McKeon P, Hertel J. (2009). Does the use of orthoses improve self-reported pain and function measures in patients with plantar fasciitis? A meta-analysis. Phys Ther Sport, 10(1):12-8. [Medline].
13) Kogler GF, Solomonidis SE, Paul JP. (1995). In vitro method for quantifying the effectiveness of the longitudinal arch support mechanism of a foot orthosis. Clin Biomech (Bristol, Avon), 10(5):245-252. [Medline]
14) Kogler GF, Solomonidis SE, Paul JP. Biomechanics of longitudinal arch support mechanisms in foot orthoses and their effect on plantar aponeurosis strain. Clin Biomech (Bristol, Avon). 1996 Jul. 11(5):243-252. [Medline].
15) Whittaker GA, Munteanu SE, Menz HB, Tan JM, Rabusin CL, Landorf KB. (2017). Foot orthoses for plantar heel pain: a systematic review and meta-analysis. Br J Sports Med. [Medline].
16) Lynch DM, Goforth WP, Martin JE, Odom RD, Preece CK, Kotter MW. (1998). Conservative treatment of plantar fasciitis. A prospective study. J Am Podiatr Med Assoc, 88:375–80.
17) Donley BG, Moore T, Sferra J, Gozdanovic J, Smith R. (2007). The efficacy of oral nonsteroidal anti-inflammatory medication (NSAID) in the treatment of plantar fasciitis: a randomized, prospective, placebo-controlled study. Foot Ankle Int, 28(1):20–3. DOI: http://dx.doi.org/10.3113/FAI.2007.0004. [PubMed] [Google Scholar]
18) Goff JD, Crawford R. (2011). Diagnosis and treatment of plantar fasciitis. Am Fam Physician, 15;84(6):676–82. [PubMed].
19) Mizel MS, Marymont JV, Trepman E. (1996). Treatment of plantar fasciitis with a night splint and shoe modification consisting of a steel shank and anterior rocker bottom. Foot Ankle Int, 17(12):732-5. [Medline].
20) Powell M, Post WR, Keener J, Wearden S. (1998). Effective treatment of chronic plantar fasciitis with dorsiflexion night splints: a crossover prospective randomized outcome study. Foot Ankle Int, 19(1):10-8. [Medline].
21) Reid DC. (1992). Sports injury assessment and rehabilitation. New York: Churchill Livingstone.
22) Elizondo-Rodriguez J, Araujo-Lopez Y, Moreno-Gonzalez JA, Cardenas-Estrada E, Mendoza-Lemus O, Acosta-Olivo C. (2013). A comparison of botulinum toxin a and intralesional steroids for the treatment of plantar fasciitis: a randomized, doubleblinded study. Foot Ankle Int, 34(1):8-14. [Medline].
23) Babcock MS, Foster L, Pasquina P, Jabbari B. (2005). Treatment of pain attributed to plantar fasciitis with botulinum toxin a: a short-term, randomized, placebo-controlled, double-blind study. Am J Phys Med Rehabil, 84(9):649-54. [Medline].
24) Huang YC, Wei SH, Wang HK, Lieu FK. (2010). Ultrasonographic guided botulinum toxin type A treatment for plantar fasciitis: an outcome-based investigation for treating pain and gait changes. J Rehabil Med, 42(2):136-40. [Medline].
25) Aqil A, Siddiqui MR, Solan M, Redfern DJ, Gulati V, Cobb JP. (2013). Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: a meta-analysis of RCTs. Clin Orthop Relat Res, 471(11):3645-52. [Medline].
26) Dizon JN, Gonzalez-Suarez C, Zamora MT, Gambito ED. (2013). Effectiveness of extracorporeal shock wave therapy in chronic plantar fasciitis: a meta-analysis. Am J Phys Med Rehabil, 92(7):606-20. [Medline].
27) Mariotto S, de Prati AC, Cavalieri E, Amelio E, Marlinghaus E, Suzuki H. (2009). Extracorporeal shock wave therapy in inflammatory diseases: molecular mechanism that triggers anti-inflammatory action. Curr Med Chem, 16(19):2366-2372.
28) Liden B, Simmons M, Landsman AS. (2009). A retrospective analysis of 22 patients treated with percutaneous radiofrequency nerve ablation for prolonged moderate to severe heel pain associated with plantar fasciitis. J Foot Ankle Surg, 48(6):642-7. [Medline]
29) Sorensen MD, Hyer CF. (2009). Bi-Polar Radiofrequency Microdebridement in the Treatment of Chronic Recalcitrant Plantar Fasciitis. Presented at the American College of Foot & Ankle Surgeons Annual Meeting, Washington, D.C
30) Boyle RA, Slater GL. (2003). Endoscopic plantar fascia release: a case series. Foot Ankle Int, 24(2):176-9. [Medline].
31) Sollitto RJ, Plotkin EL, Klein PG, Mullin P. (1997). Early clinical results of the use of radiofrequency lesioning in the treatment of plantar fasciitis. J Foot Ankle Surg, 36(3):215-9; discussion 256. [Medline].
32) Bazaz R, Ferkel RD. (2007). Results of endoscopic plantar fascia release. Foot Ankle Int, 28(5):549-56. [Medline].
33) Cavazos GJ, Khan KH, D’Antoni AV, Harkless LB, Lopez D. (2009). Cryosurgery for the treatment of heel pain. Foot Ankle Int, 30(6):500-5. [Medline].
More Plantar Fasciitis Topics to Explore
| Causes | Natural Treatments | Finding a Doctor |
| Surgery | Fitness | Shoes |
| Sudden Plantar Fasciitis | Morning Heel Pain | Plantar Fascia Ligament |

